Endostory No.17: Carcinoid tumor or adenocarcinoma? A lesson from a small cardia lesion
A small lesion, just over 1 cm in the cardia, initially appeared to be a benign carcinoid tumor. However, behind this seemingly straightforward image, histopathology told a completely different story. Follow ENDOSTORY #17 and discover how “small and innocent” lesions can sometimes become the ultimate test of an endoscopist’s observational and diagnostic skills.
Initial clinical findings
A 79-year-old female patient with an unremarkable medical history presented with epigastric pain. Endoscopic examination revealed a tumor in the cardia region.
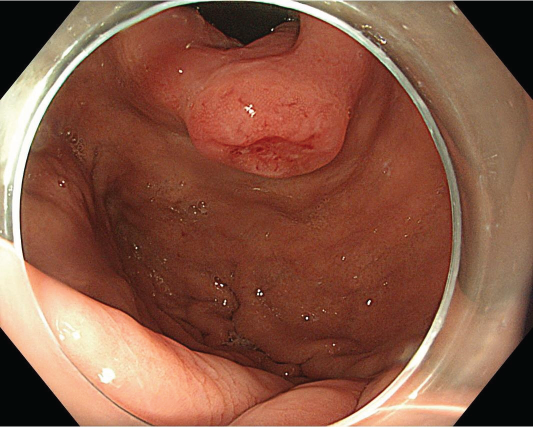
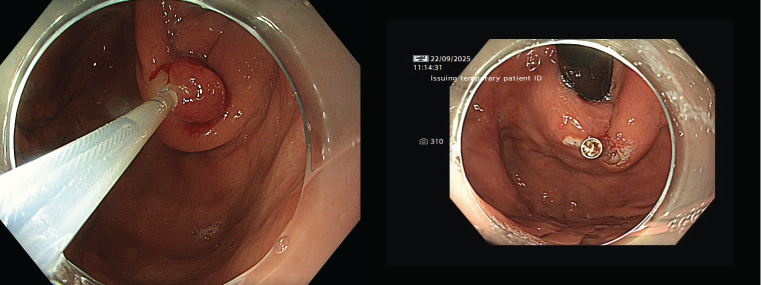
Under white-light observation, a slightly reddish lesion approximately 10 mm in diameter was detected at the cardia. The lesion appeared mildly elevated with a central depression, suggesting a submucosal tumor.
The mucosa surrounding the lesion showed prominent vascular dilatation, indicating localized hyperemia. Due to the difficult access and limited visualization angle at the cardia, detailed observation of the central depression under standard white light was not possible.
Diagnosis
Based on the endoscopic findings and lesion characteristics, the patient was provisionally diagnosed with a suspected carcinoid tumor of the gastric cardia. The lesion’s elevated morphology with a mild central depression and a size of about 1 cm were consistent with typical carcinoid features.
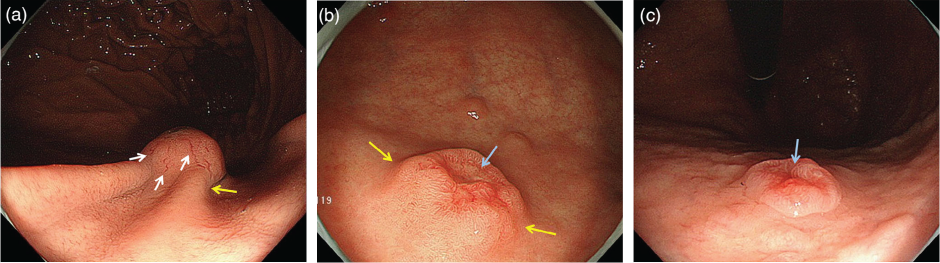
Typical endoscopic characteristics of a carcinoid tumor in the cardia include:
- Dilated blood vessels (a)
- Submucosal tumor-like protrusion (b)
- Characteristic central depression (c)
In this case, differential diagnosis included adenocarcinoma, as the central area showed irregular surface and abnormal vascular patterns. However, given the small size (≤1 cm), the lesion was considered more likely to be a carcinoid tumor, and an endoscopic intervention was planned.

ESD intervention and results
With the working diagnosis of a small carcinoid tumor, the patient underwent endoscopic tumor removal using the hot snare polypectomy technique. The procedure lasted about 15 minutes.
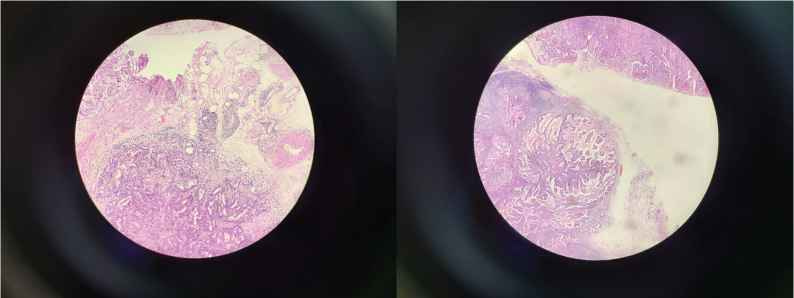
Histopathological results revealed a moderately differentiated adenocarcinoma, classified as pT1b — cancer cells had invaded the submucosa, but there was no evidence of vascular invasion (v0) or lymphatic invasion (ly0).
However, the horizontal margin (HM1) was positive for cancer cells, while the vertical margin (VM0) was negative, indicating possible residual tumor tissue at the horizontal resection margin.
Based on these findings, surgical intervention was recommended as the next step.
Conclusion
Gastric carcinoid tumors often present with quite characteristic endoscopic features — a slightly reddish, elevated lesion with a central depression and surrounding dilated vessels. However, in some cases, especially when the central depressed area shows irregular microvessels or abnormal surface patterns, distinguishing between carcinoid tumor and adenocarcinoma can be challenging.
Therefore, biopsy of the central depressed area plays a crucial role in accurate diagnosis. Proper sampling allows determination of the lesion’s nature, helping clinicians establish an appropriate treatment strategy — avoiding both the risk of missing early invasive adenocarcinoma and the risk of overtreatment of a benign carcinoid tumor.