ENDOSTORY No.12: Kyoto classification – “The map” guiding from gastric endostory images to clinical decisions
Initiated by the Japan Gastroenterological Endoscopy Society (JGES), the Kyoto Classification was introduced in 2013 as a “common language” for endoscopists to evaluate gastric mucosal endoscopic images and make accurate risk assessments. Instead of vaguely describing gastritis as before, this system defines 5 key features—atrophy, intestinal metaplasia, enlarged folds, nodularity, and diffuse redness with or without regular arrangement of collecting venules (RAC)—to assign a score ranging from 0 to 8.
The Kyoto score not only predicts H. pylori infection status but also stratifies gastric cancer risk. Along with advances in modern endoscopy (such as NBI), these features are increasingly clarified, making the Kyoto Classification a simple yet highly valuable clinical tool. Let’s join ENDOSTORY #12 and Lenus Vietnam in exploring the role of Kyoto Classification in gastric cancer diagnosis.
Overview of the Kyoto Classification
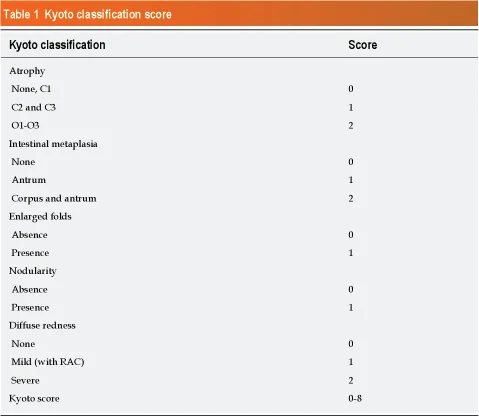
The Kyoto Classification is an endoscopic system designed to define findings associated with H. pylori infection. It is based on 5 main endoscopic features, each scored from 0–2 points, with a total score ranging from 0 to 8, including:
- Atrophy: 0 points if absent or C1, 1 point for C2–C3, 2 points for O1–O3
- Intestinal metaplasia: 0 points if absent, 1 point when limited to the antrum, 2 points when extending to the corpus
- Enlarged folds: 0 points if absent, 1 point if present
- Nodularity: 0 points if absent, 1 point if present
- Diffuse redness: 0 points if absent, 1 point if mild with RAC, 2 points if severe or RAC loss
Accordingly:
- A total score of 0 usually suggests H. pylori negative.
- A total score ≥2 suggests ongoing H. pylori infection.
- A total score ≥4 is associated with higher gastric cancer risk and requires close monitoring.
Thus, the Kyoto Classification is structured around 5 standardized endoscopic features for scoring and risk stratification. (It should be noted that, in clinical practice, other endoscopic features—about 19 in total—are also linked to chronic H. pylori-related gastritis, such as atrophy, intestinal metaplasia, enlarged folds, nodularity, map-like redness, xanthoma, mucosal edema, red streaks, fundic gland polyps, etc. However, only the 5 main features are standardized for Kyoto scoring, while the others serve as supplementary findings.)
Atrophy and the Kimura–Takemoto Classification
In the Kyoto Classification, atrophy is one of the most important features for risk evaluation. Atrophy is assessed both histologically and endoscopically.
- Histologically, atrophy is defined as the loss of glandular structures.
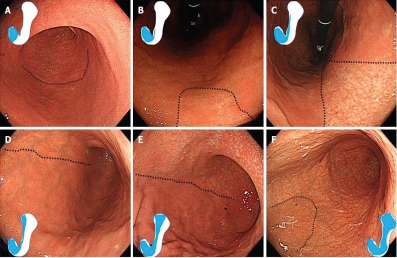
- Endoscopically, atrophy is evaluated using the Kimura–Takemoto classification, a classic system from Japan. Endoscopic atrophy is characterized by visible vascular networks, pale-yellow discoloration, and reduced mucosal height. In contrast, areas with diffuse redness lack atrophy.
Kimura–Takemoto divides atrophy into closed type (C1–C3) and open type (O1–O3), reflecting the spread from antrum to corpus. The Kyoto system converts this as follows:
- C0/C1 = 0 points (no or minimal atrophy)
- C2–C3 = 1 point (moderate atrophy)
- O1–O3 = 2 points (extensive atrophy)
The classification implies that the more extensive the atrophy, the higher the risk of gastric cancer—even after H. pylori eradication. Therefore, accurate recognition and classification of atrophy are essential when applying the Kyoto system for risk stratification.
Intestinal Metaplasia and Scoring in the Kyoto Classification
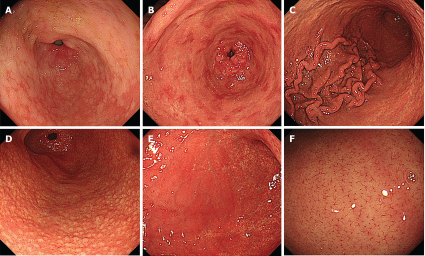
Intestinal metaplasia (IM) typically appears endoscopically as whitish-gray, slightly elevated plaques surrounded by pale pink mucosa, creating a rough, irregular surface.
Modern image-enhanced endoscopy techniques such as NBI, BLI, and LCI improve detection and diagnostic accuracy of IM. Under magnifying NBI (M-NBI), the presence of white opaque substance (WOS) and light blue crests are strong indicators of IM.
In the Kyoto Classification, IM is scored as follows:
- 0 points: no IM
- 1 point: IM limited to the antrum
- 2 points: IM extending to the corpus
Application of the Kyoto Classification: Diagnosing H. pylori Infection
One important application of the Kyoto Classification is diagnosing H. pylori infection during endoscopy without necessarily relying on biopsy tests.
- Kyoto score = 0 strongly correlates with H. pylori negative.
- Kimura score ≥2 (O-type atrophy) suggests past or ongoing H. pylori infection.
Key endoscopic features:
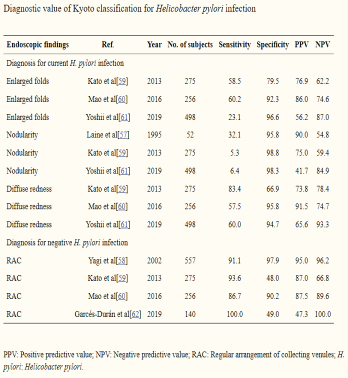
- Enlarged folds: positive predictive value (PPV) 56–86% for H. pylori infection.
- Nodularity: rare but highly specific (>95%), almost always indicating infection when present.
- Diffuse redness: PPV 65.6–91.5%, commonly seen in active H. pylori gastritis.
- RAC: well-preserved RAC strongly suggests H. pylori negative, with high sensitivity and specificity across studies.
Application of the Kyoto Classification: Predicting Gastric Cancer Risk
Perhaps the most clinically significant value of the Kyoto Classification is predicting gastric cancer risk based on the degree of endoscopic atrophy.
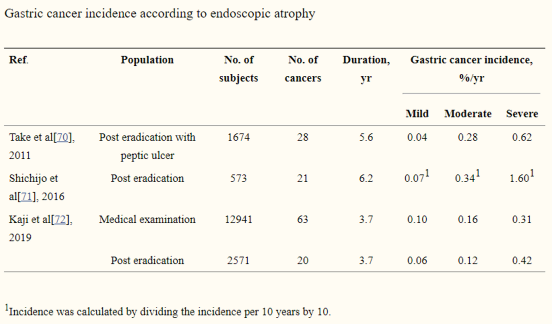
Studies show a clear correlation: the more severe the atrophy, the higher the risk of gastric cancer. Atrophy disrupts normal glandular architecture, replaces it with fibrous tissue, and is often accompanied by intestinal metaplasia/dysplasia—precursors of carcinogenesis. Thus, endoscopic assessment of atrophy is a key step in predicting and stratifying gastric cancer risk.
Even after H. pylori eradication, patients with severe atrophy remain at elevated risk.
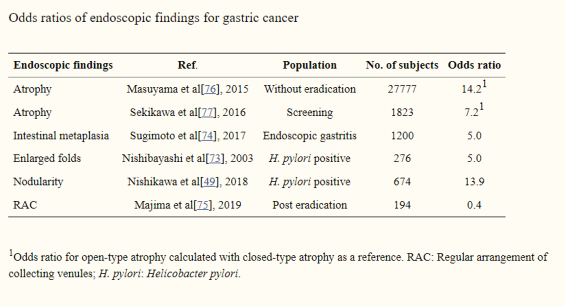
Associations between Kyoto features and gastric cancer risk (OR values):
- Atrophy: OR 7.2–14.2 → extensive atrophy increases cancer risk 7–14 fold.
- Intestinal metaplasia: OR ~5.0 → an important precancerous lesion requiring close follow-up.
- Enlarged folds: OR ~5.0 → associated with active H. pylori inflammation.
- Nodularity: OR ~13.9 → very high risk, reflecting long-standing active gastritis.
- RAC: OR ~0.4 → presence of RAC is protective, seen in H. pylori-negative or well-healed mucosa.
Conclusion
The Kyoto Classification provides not only a standardized descriptive system for gastric endoscopic findings but also a practical clinical tool to diagnose H. pylori infection and predict gastric cancer risk. It can be regarded as a “guiding map” enabling endoscopists to visualize, interpret, and foresee the future of a patient’s stomach. Thorough recording and reporting of Kyoto features contribute significantly to strategies for prevention and early detection of gastric cancer, supporting long-term, comprehensive patient care.
About the ENDOSTORY Series
ENDOSTORY is a clinical endoscopy case-sharing series conducted by Lenus Vietnam, aiming to provide valuable information for endoscopists. Every week, one carefully selected “story” is published on the Lenus Vietnam fanpage at 8:00 PM on Fridays.
The series is supervised by Dr. Trần Đức Cảnh – a specialist in early cancer diagnosis and treatment. Not only directly involved in numerous complex ESD cases, Dr. Cảnh is also a dedicated mentor, training many young Vietnamese endoscopists in ESD, helping to spread this “golden key” technique for early gastrointestinal cancer treatment. His spirit of sharing and dedication has been an inspiration for the creation of the ENDOSTORY journey.